









The History of Botulinum Toxin
The history of Botulinum Toxin, often referred to as “botox”, is a fascinating journey that spans over several decades. This potent neurotoxin, produced by the bacterium Clostridium botulinum, has found its place in the world of cosmetic dermatology, offering a non-surgical solution to a variety of aesthetic concerns.
The discovery of Botulinum Toxin dates back to the 19th century when a German physician, Justinus Kerner, first identified it while investigating a series of food poisoning cases. Kerner coined the term “botulism” from the Latin word for sausage, “botulus,” as the affected individuals had consumed improperly prepared sausages. He was the first to recognize the paralytic symptoms of botulism and postulated the existence of a “fatty poison” that interfered with the transmission of nerve impulses.
In the early 20th century, Emile Pierre van Ermengem, a Belgian bacteriologist, isolated the bacterium we now know as Clostridium botulinum. He discovered that the bacterium produced a toxin that caused the symptoms of botulism. This marked the first step in understanding the nature of this potent neurotoxin.
The therapeutic potential of Botulinum Toxin was not realized until the mid-20th century. During the 1940s and 1950s, scientists at the United States Army’s biological warfare laboratories at Fort Detrick, Maryland, conducted extensive research on Botulinum Toxin as a potential biological weapon. Although the military applications of the toxin were never fully realized, this research paved the way for understanding the toxin’s therapeutic potential.
In the 1960s, Dr. Alan B. Scott, an ophthalmologist, began investigating the potential use of Botulinum Toxin to treat strabismus (crossed eyes), a condition that was difficult to treat surgically. His research led to the development of a purified and diluted form of the toxin that could be injected into muscles to cause temporary paralysis. In 1989, the U.S. Food and Drug Administration (FDA) approved the use of Botulinum Toxin type A (marketed as Botox) for the treatment of strabismus and blepharospasm (uncontrolled blinking).
The cosmetic applications of Botulinum Toxin were discovered somewhat serendipitously. Jean Carruthers, a Canadian ophthalmologist, noticed that her patients who received Botox treatments for eye disorders also experienced improvement in facial wrinkles. This observation led to a series of studies conducted by Jean and her husband, Alastair Carruthers, a dermatologist, which eventually led to the FDA approval of Botox for cosmetic use in 2002.
Since then, the use of Botulinum Toxin in cosmetic dermatology has skyrocketed. It is now used to treat a variety of conditions, including forehead wrinkles, crow’s feet, and frown lines. The toxin works by blocking the nerve signals to the muscles, causing them to relax and reducing the appearance of wrinkles.
The journey of Botulinum Toxin from a deadly poison to a beloved wrinkle reducer is a testament to the power of scientific research and innovation. As our understanding of this potent neurotoxin continues to grow, so too will its applications in cosmetic dermatology and beyond.
Different Botulinum Toxins
BOTOX Cosmetic (onabotulinumtoxinA):

Indication
This drug is used in adults for temporary improvement in the appearance of moderate to severe glabellar lines (lines between the eyebrows) associated with corrugator and/or procerus muscle activity. It is also indicated for the treatment of moderate to severe lateral canthal lines (crow’s feet) associated with orbicularis oculi activity, and moderate to severe forehead lines associated with frontalis muscle activity.
Dilution
This drug is supplied in single-dose 50 Units and 100 Units per vial. It should be reconstituted with sterile, preservative-free 0.9% Sodium Chloride Injection USP to obtain a solution at a concentration of 4 Units/0.1 mL. The reconstituted BOTOX Cosmetic should be clear, colorless, and free of particulate matter. It should be administered within 24 hours after reconstitution and stored in a refrigerator during this time period. The vials are for single-dose only.
Administration
The drug is administered intramuscularly into five sites, two each corrugator muscle and one in the procerus muscle for a total dose of 20 Units. The dosage for simultaneous treatment with lateral canthal lines is 64 Units, comprised of 20 Units for forehead lines, 20 Units for glabellar lines, and 24 Units for lateral canthal lines. The drug should be administered no closer than 1 cm above the central eyebrow to reduce the risk of ptosis.
Storage
The product is supplied as a vacuum-dried powder in single-dose vials of 50 or 100 Units. Unopened vials should be stored in a refrigerator (2° to 8°C). Reconstituted BOTOX Cosmetic should also be stored in a refrigerator and used within 24 hours.
DYSPORT (abobotulinumtoxinA):

Indication
This drug is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with procerus and corrugator muscle activity in adults less than 65 years of age.
Dilution
This drug is supplied as a dry powder in single-dose 300 Unit and 500 Unit vials. It should be reconstituted with preservative-free 0.9% Sodium Chloride Injection, USP using aseptic technique. The reconstituted DYSPORT should be a clear, colorless solution, free of particulate matter. It should be used for only one injection session and for only one patient. Once reconstituted, it can be stored in a refrigerator, protected from light for up to 24 hours until time of use.
Administration
The dose for the treatment of glabellar lines in adults is a total of 50 Units given intramuscularly in five equal aliquots of 10 Units each to achieve clinical effect. The drug should be administered no more frequently than every three months. To reduce the risk of ptosis, the drug should be injected at least 1 centimeter above the bony supraorbital ridge and no closer than 1 centimeter above the central eyebrow.
Storage
This is supplied as a sterile, lyophilized powder in a single-dose, glass vial. Unopened vials must be stored refrigerated (2°C to 8°C) and protected from light.
XEOMIN (incobotulinumtoxinA):

Indication
It is indicated for temporary improvement in the appearance of moderate to severe glabellar lines with corrugator and/or procerus muscle activity.
Dilution
It should be reconstituted with only 2.5mL sterile, preservative-free 0.9% Sodium Chloride Injection, USP to obtain a solution at a concentration of 4 Units/0.1 mL. The frequency of XEOMIN treatments should be no sooner than every 12 weeks.
Administration
The drug is administered intramuscularly into five sites, two injections into medial corrugator and lateral corrugator muscles respectively, and one injection in the procerus muscle for a total dose of 20 Units. To reduce the risk of ptosis, the drug should be injected no less than 1 centimeter above the superior orbital rim.
Storage
Supplied in single-dose vials of 50, 100, or 200 Units. Unopened vials can be stored at room temperature (20°C to 25°C), in a refrigerator (2°C to 8°C), or a freezer (-20°C to -10°C). Reconstituted XEOMIN should not be used if the solution appears cloudy or contains particulate matter, and any unused solution should be discarded after 24 hours.
JEUVEAU (prabotulinumtoxinA-xvfs):

Indication
This drug is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with corrugator and/or procerus muscle activity in adult patients.
Dilution
This drug is supplied in a single-dose 100 Unit vial. It should be reconstituted with only 2.5mL sterile, preservative-free 0.9% Sodium Chloride Injection, USP to obtain a solution at a concentration of 4 Units/0.1 mL. The reconstituted JEUVEAU should be clear, colorless, and free of particulate matter. It should be administered within 24 hours after reconstitution and stored in a refrigerator during this time period. The vials are for single-dose only.
Administration
The drug is administered intramuscularly into five sites, two injections into medial corrugator and lateral corrugator muscles respectively, and one injection in the procerus muscle for a total dose of 20 Units. To reduce the risk of ptosis, the drug should be injected no less than 1 centimeter above the superior orbital rim.
Storage
Supplied as a vacuum-dried powder in a single-dose vial of 100 Units. Unopened vials should be stored in a refrigerator (2° to 8°C) and protected from light.
DAXXIFY (daxibotulinumtoxinA-lanm)

Indication
This drug is indicated for the temporary improvement in the appearance of moderate to severe glabellar lines associated with corrugator and/or procerus muscle activity in adult patients.
Dilution
This drug is supplied in single-dose 50 Unit and 100 Unit vials. It should be reconstituted with the required amount of sterile, preservative-free 0.9% Sodium Chloride Injection, USP to obtain a solution at a concentration of 8 Units/0.1 mL. The reconstituted DAXXIFY solution should be clear to slightly opalescent and colorless and free of particulate matter. It should be administered within 72 hours after reconstitution and stored in a refrigerator during this time period.
Administration
The drug is administered intramuscularly into five sites, two injections into medial corrugator and lateral corrugator muscles respectively, and one injection in the procerus muscle for a total dose of 40 Units. To reduce the risk of ptosis, the drug should be injected no less than 1 centimeter above the superior orbital rim.
Storage
Supplied as a sterile lyophilized powder in single-dose vials of 50 or 100 Units. Unopened vials should be stored at room temperature (20°C to 25°C) or refrigerated (2°C to 8°C) and protected from light.
General Contraindications
Botulinum toxin drugs are contraindicated in patients with:
Known hypersensitivity to any botulinum toxin products or to any of the components in the formulation. This includes specific hypersensitivity to cow’s milk protein, which may be present in trace amounts in some formulations.
Presence of infection at the proposed injection site(s).
These contraindications apply to all the mentioned botulinum toxin drugs: BOTOX Cosmetic, DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY.
Warnings and Precautions
Lack of Interchangeability between Botulinum Toxin Products
The potency units of botulinum toxin products, including BOTOX Cosmetic (onabotulinumtoxinA), DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY (daxibotulinumtoxinA-lanm), are specific to the preparation and assay method utilized. They are not interchangeable with other preparations of botulinum toxin products. Therefore, units of biological activity of these products cannot be compared to nor converted into units of any other botulinum toxin products assessed with any other specific assay method.
Spread of Toxin Effect:
Postmarketing safety data from botulinum toxin products, including BOTOX Cosmetic, DYSPORT, XEOMIN, JEUVEAU, and DAXXIFY, suggest that botulinum toxin effects may, in some cases, be observed beyond the site of local injection. The symptoms are consistent with the mechanism of action of botulinum toxin and may include asthenia, generalized muscle weakness, diplopia, blurred vision, ptosis, dysphagia, dysphonia, dysarthria, urinary incontinence, and breathing difficulties.
These symptoms have been reported hours to weeks after injection. Swallowing and breathing difficulties can be life-threatening, and there have been reports of death related to the spread of toxin effects. Patients should be advised to seek immediate medical care if swallowing, speech, or respiratory difficulties occur. Although no serious adverse reactions of distant spread of toxin effect associated with these products have been reported in clinical studies for their specific approved indications, these reactions are possible.
Serious adverse reactions with unapproved use:
Serious adverse reactions, including excessive weakness, dysphagia, and aspiration pneumonia, with some adverse reactions associated with fatal outcomes, have been reported in patients who received botulinum toxin injections for unapproved uses. These adverse reactions were not necessarily related to distant spread of toxin, but may have resulted from the administration of botulinum toxin products to the site of injection and/or adjacent structures. In several cases, patients had pre-existing dysphagia or other significant disabilities. There is insufficient information to identify factors associated with an increased risk for adverse reactions associated with the unapproved uses of botulinum toxin products. The safety and effectiveness of botulinum toxin for unapproved uses have not been established.
Hypersensitivity Reactions:
Serious and/or immediate hypersensitivity reactions have been reported for botulinum toxin products. These reactions include anaphylaxis, serum sickness, urticaria, soft tissue edema, and dyspnea. If such a reaction occurs, further injection of the botulinum toxin product should be discontinued and appropriate medical therapy immediately instituted. The use of botulinum toxin products in patients with a known hypersensitivity to any botulinum neurotoxin or to any of the components in the formulation could lead to a life-threatening allergic reaction.
Cardiovascular System:
There have been reports following administration of botulinum toxins of adverse events involving the cardiovascular system, including arrhythmia and myocardial infarction, some with fatal outcomes. Some of these patients had risk factors including pre-existing cardiovascular disease. Use caution when administering to patients with pre-existing cardiovascular disease.
Increased Risk with Pre-Existing Neuromuscular Disorders:
Individuals with peripheral motor neuropathic diseases, amyotrophic lateral sclerosis, or neuromuscular junction disorders (e.g., myasthenia gravis or Lambert-Eaton syndrome) should be monitored particularly closely when given botulinum toxin. Patients with neuromuscular disorders may be at increased risk of clinically significant effects including generalized muscle weakness, diplopia, ptosis, dysphonia, dysarthria, severe dysphagia, and respiratory compromise.
Dysphagia and Breathing Difficulties:
Treatment with botulinum toxin products can result in swallowing or breathing difficulties. Patients with pre-existing swallowing or breathing difficulties may be more susceptible to these complications. In most cases, this is a consequence of weakening of muscles in the area of injection that are involved in breathing or swallowing. Deaths as a complication of severe dysphagia have been reported after treatment with botulinum toxin. Dysphagia may persist for several months, and require use of a feeding tube to maintain adequate nutrition and hydration. Aspiration may result from severe dysphagia and is a particular risk when treating patients in whom swallowing or respiratory function is already compromised. Treatment with botulinum toxins may weaken neck muscles that serve as accessory muscles of ventilation. This may result in a critical loss of breathing capacity in patients with respiratory disorders who may have become dependent upon these accessory muscles. There have been postmarketing reports of serious breathing difficulties, including respiratory failure. Patients treated with botulinum toxin may require immediate medical attention should they develop problems with swallowing, speech or respiratory disorders. These reactions can occur within hours to weeks after injection with botulinum toxin.
Pre-existing Conditions at the Injection Site:
Caution should be used when botulinum toxin treatment is used in the presence of inflammation at the proposed injection site(s), ptosis, or when excessive weakness or atrophy is present in the targeted muscle(s). This also applies to patients who have marked facial asymmetry, excessive dermatochalasis, deep dermal scarring, thick sebaceous skin, or when subjects do not respond to 20 Units of botulinum toxin (e.g., the inability to substantially lessen glabellar lines even by physically spreading them apart). Use caution when administering to patients with surgical alterations to the facial anatomy. Do not exceed the recommended dosage and frequency of administration.
Corneal Exposure and Ulceration:
This may require protective drops, ointment, or closure of the eye by patching or other means. Because of its anticholinergic effects, botulinum toxin should be used with caution in patients at risk of developing narrow angle glaucoma. To prevent ectropion, botulinum toxin products should not be injected into the medial lower eyelid area. Ecchymosis easily occurs in the soft tissues of the eyelid. Immediate gentle pressure at the injection site can limit that risk.
Ophthalmic Adverse Reactions:
Dry Eye:
Dry eye has been reported with the use of botulinum toxin products in the treatment of glabellar lines. Reduced tear production, reduced blinking, and corneal disorders may occur with use of botulinum toxins. If symptoms of dry eye (e.g., eye irritation, photophobia, or visual changes) persist, consider referring the patient to an ophthalmologist.
Spatial Disorientation and Double Vision Treated for Strabismus:
Inducing paralysis in one or more extraocular muscles may produce spatial disorientation, or double vision.. Covering the affected eye may alleviate these symptoms.
Human Albumin and Transmission of Viral Diseases:
The product contains albumin, a derivative of human blood. Based on effective donor screening and product manufacturing processes, it carries an extremely remote risk for transmission of viral diseases and variant Creutzfeldt-Jakob disease (vCJD). There is a theoretical risk for transmission of Creutzfeldt-Jakob disease (CJD), but if that risk actually exists, the risk of transmission would also be considered extremely remote. No cases of transmission of viral diseases, CJD or vCJD have ever been identified for licensed albumin or albumin contained in other licensed products.
Facial Anatomy in the Treatment of Glabellar Lines:
Caution should be exercised when administering botulinum toxin to patients with surgical alterations to the facial anatomy, excessive weakness or atrophy in the target muscle(s), marked facial asymmetry, inflammation at the injection site(s), ptosis, excessive dermatochalasis, deep dermal scarring, thick sebaceous skin, or the inability to substantially lessen glabellar lines by physically spreading them apart. Do not exceed the recommended dosage and frequency of administration. In clinical trials, subjects who received a higher dose had an increased incidence of eyelid ptosis.
Intradermal Immune Reaction:
The possibility of an immune reaction when injected intradermally is unknown. The safety of botulinum toxin for the treatment of hyperhidrosis has not been established. It is approved only for intramuscular injection.
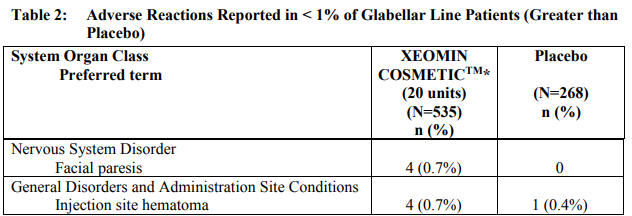
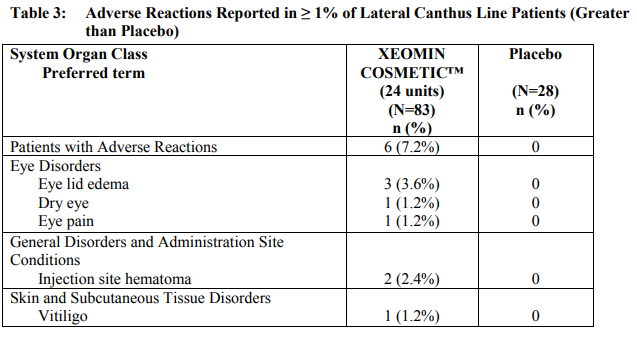
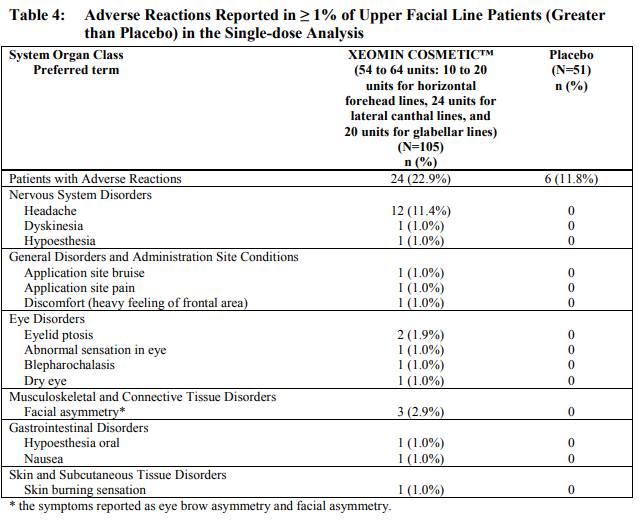
Side Effects/ Adverse Reactions
Here is the list of major side effects taken from the Xeomin, botulinum toxin. Most botulinum toxin share similar side effect / adverse event profile. Please check your package insert for a detailed list.

Immunogenicity
As with all therapeutic proteins, there is a potential for immunogenicity. The detection of antibody formation is highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody (including neutralizing antibody) positivity in an assay may be influenced by several factors including assay methodology, sample handling, timing of sample collection, medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to botulinum toxin in different studies or to other products may be misleading.
Treatment with botulinum toxins may result in the formation of neutralizing antibodies that may reduce the effectiveness of subsequent treatments by inactivating the biological activity of the toxin. The critical factors for neutralizing antibody formation have not been well characterized. The results from some studies suggest that botulinum toxin injections at more frequent intervals or at higher doses may lead to a greater incidence of antibody formation.
Originally published at Botox Training Houston























